A collapsed lung sounds like one thing. It isn’t. The term actually covers two distinct conditions — pneumothorax, where air leaks into the chest cavity and compresses the lung, and atelectasis, where the lung tissue itself deflates due to a blockage or external pressure. Mixing them up isn’t just a semantic problem; the causes, urgency levels, and treatments are fundamentally different.

Complete guide to Collapsed Lung — Collapsed Lung: Symptoms, Causes & Treatment
Symptoms range from a mild, easy-to-dismiss ache in a healthy 20-year-old to a life-threatening emergency that can kill within minutes. Knowing which end of that spectrum you’re dealing with — and when to call 911 versus when to wait and monitor — can genuinely be the difference between a routine outpatient procedure and a critical intervention.
What follows covers the full picture: how to tell pneumothorax from atelectasis, who is most at risk and why, how doctors diagnose and treat each type, what realistic recovery actually looks like, and how to reduce the odds of it happening again.
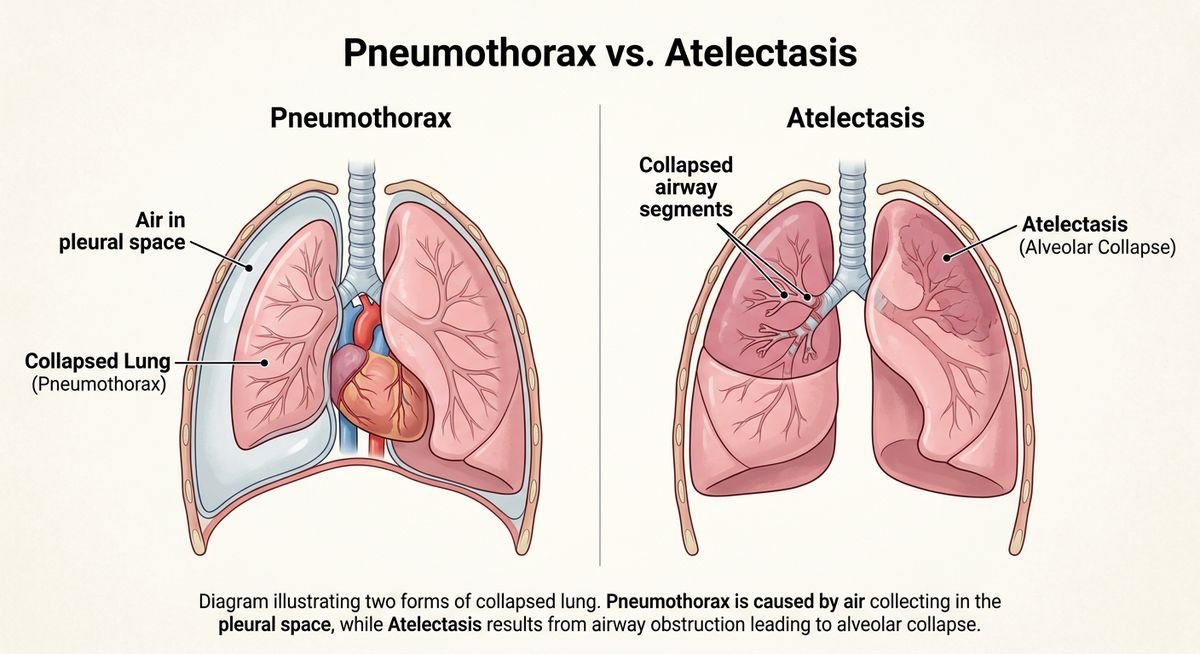
Pneumothorax vs. Atelectasis: Two Types of Collapsed Lung
Pneumothorax and atelectasis are both forms of lung collapse, but they have completely different causes, danger levels, and treatments. Pneumothorax involves air leaking into the space around the lung, while atelectasis involves airways becoming blocked or compressed until lung tissue deflates. Confusing the two — which most general sources do — can leave patients genuinely unsure about how serious their diagnosis is.
What Is Pneumothorax?
A pneumothorax occurs when air escapes into the pleural cavity — the normally airtight space between the lung and the chest wall. That air buildup exerts pressure on the lung, causing it to partially or fully collapse. The lung isn’t blocked from the inside; it’s being crushed from the outside.
There are three main subtypes. A primary spontaneous pneumothorax happens without any obvious injury or underlying disease — most commonly in tall, thin young men whose lung tissue develops small air-filled blisters called blebs that rupture without warning. A secondary spontaneous pneumothorax occurs in people with pre-existing lung disease like COPD, asthma, or cystic fibrosis, and tends to be far more serious because the lungs are already compromised. A traumatic pneumothorax results from a direct physical injury — a car accident, a stab wound, or even a broken rib puncturing the lung.
The most dangerous variant is tension pneumothorax. Air enters the pleural space but has no way to escape, creating a one-way valve effect that progressively compresses not just the lung but the heart and major blood vessels. Blood pressure drops. Oxygen delivery collapses. This is a medical emergency requiring a 911 call and intervention within minutes — not hours.
What Is Atelectasis?
Atelectasis is a different mechanism entirely. Here, lung tissue deflates because airways become blocked — by mucus, a tumor, an inhaled object, or external compression from fluid or a tumor pressing against the lung. Without airflow reaching those sections, the affected tissue simply collapses inward.
Atelectasis is most often a complication of something else rather than a standalone emergency. According to the American Thoracic Society, it is one of the most common post-surgical respiratory complications, particularly after abdominal or thoracic procedures where shallow breathing and immobility allow mucus to accumulate and plug smaller airways. Prolonged bed rest carries the same risk.
Symptoms can overlap with pneumothorax — shortness of breath, reduced oxygen levels, a dull chest discomfort — but atelectasis rarely produces the sudden, sharp one-sided chest pain that typically signals a pneumothorax. Treatment also diverges sharply: pneumothorax often requires needle aspiration or a chest tube to remove trapped air, while atelectasis is typically managed with breathing exercises, chest physiotherapy, bronchoscopy to clear blockages, or treating the underlying cause.
| Feature | Pneumothorax | Atelectasis |
|---|---|---|
| Core mechanism | Air in pleural space compresses the lung | Blocked or compressed airway deflates lung tissue |
| Typical onset | Sudden, often without warning | Gradual, commonly post-surgical |
| Primary treatment | Needle aspiration or chest tube | Breathing exercises, bronchoscopy |
| Emergency potential | High (tension pneumothorax can be fatal) | Low to moderate |
| Recurrence risk | 30-50% within 1-3 years without surgery | Depends on underlying condition |
Symptoms and Warning Signs
A collapsed lung most commonly announces itself with sudden, sharp chest pain on one side and shortness of breath that arrives without warning — sometimes mid-sentence, sometimes mid-sleep. Symptoms range from surprisingly subtle to life-threatening within minutes, depending entirely on the type and size of the collapse.
Common Symptoms
The hallmark presentation is unilateral chest pain — one-sided, often described as stabbing or tearing — accompanied by breathlessness that worsens with any physical effort. A rapid heart rate (tachycardia) typically follows as the body compensates for reduced oxygen exchange. On clinical examination, breath sounds are diminished or absent on the affected side, a finding doctors can detect with a stethoscope in seconds.
Severity varies dramatically by patient profile. In primary spontaneous pneumothorax — the kind that strikes otherwise healthy young adults — symptoms can feel mild enough to dismiss as a pulled muscle or anxiety. Many patients wait hours or even days before seeking care. Secondary spontaneous pneumothorax in someone with underlying COPD or asthma is a different story entirely: the same volume of air leak causes immediate, severe respiratory distress because the remaining lung function is already compromised.
Atelectasis, the other form of collapsed lung, tends to produce a quieter symptom picture — low-grade breathlessness, mild chest tightness, and sometimes a low fever, particularly post-surgery. It rarely causes the sudden stabbing pain associated with pneumothorax.
| Symptom | Pneumothorax | Atelectasis |
|---|---|---|
| Chest pain | Sudden, sharp, one-sided | Mild or absent |
| Shortness of breath | Moderate to severe | Mild to moderate |
| Onset | Abrupt | Gradual |
| Breath sounds | Reduced on affected side | Diminished, often diffuse |
| Fever | Rare | Possible (especially post-op) |
When to Call 911
Emergency Warning: Tension Pneumothorax Red Flags
Tension pneumothorax is not a “wait and see” situation. It is a rapidly fatal emergency in which trapped air builds pressure with every breath, compressing the heart and opposite lung. Death can occur within minutes without immediate intervention. Call 911 if you or someone nearby shows any of the following:
- Breathing that worsens rapidly despite sitting still or resting
- Bluish lips, fingertips, or face (cyanosis) — a sign of critical oxygen deprivation
- Falling blood pressure combined with a racing pulse
- Tracheal deviation — the visible or palpable shift of the windpipe away from center
- Confusion, agitation, or loss of consciousness
- Neck vein distension (jugular venous distension)
These signs require emergency intervention within minutes, not hours. According to the American College of Emergency Physicians, tension pneumothorax is one of the leading causes of preventable cardiac arrest in trauma patients. Emergency physicians typically perform needle decompression — inserting a large-bore needle into the second intercostal space — before a chest tube can be placed. Every minute of delay increases the risk of cardiovascular collapse.
Causes and Risk Factors by Demographic
A collapsed lung doesn’t strike randomly. Who you are — your age, body type, medical history, and daily habits — determines your actual risk profile far more precisely than any generic list of causes.
Who Is Most at Risk?
Primary spontaneous pneumothorax has a strikingly specific target: tall, thin males between 15 and 34 years old. The prevailing explanation is that rapid height growth outpaces lung tissue development, leaving small air-filled sacs called blebs on the lung surface — and blebs can rupture without warning, even during sleep. According to the American Thoracic Society, primary spontaneous pneumothorax occurs at a rate of roughly 7.4 per 100,000 men annually, compared to approximately 1.2 per 100,000 women.
Secondary spontaneous pneumothorax follows a different patient profile entirely. Smokers, and patients living with COPD, asthma, or cystic fibrosis, face elevated risk because underlying lung damage creates structural weak points. The longer someone has smoked, the higher the risk — smoking increases pneumothorax likelihood by a factor of roughly 20 in men, according to published pulmonology literature.
| Pneumothorax Type | Primary Demographic | Key Risk Factor |
|---|---|---|
| Primary Spontaneous | Tall, thin males, ages 15-34 | Subpleural blebs, rapid growth |
| Secondary Spontaneous | Adults 45+ with lung disease | COPD, asthma, cystic fibrosis, smoking |
| Traumatic | Any age, trauma victims | Car accidents, stab wounds, rib fractures |
| Iatrogenic | Hospitalized or ICU patients | Mechanical ventilation, central line placement |
| Pregnancy-Associated | Women in third trimester | Diaphragm elevation, hormonal changes |
Traumatic pneumothorax can happen to anyone — a high-speed car collision, a penetrating stab wound, or even a fractured rib from a hard fall can all introduce air into the pleural space. Iatrogenic pneumothorax, caused by medical procedures like mechanical ventilation or central venous catheter insertion, is a recognized hospital complication that clinicians actively monitor for in ICU settings.
Two groups that often go unmentioned deserve specific attention. Pregnant women face elevated risk in the third trimester as the growing uterus displaces the diaphragm upward, increasing pleural pressure. Patients with Marfan syndrome — a connective tissue disorder — are disproportionately affected due to the same tall, lean body morphology combined with inherently weaker tissue structure.
Lifestyle and Activity Triggers
Scuba diving is one of the highest-risk recreational activities for anyone with a history of blebs. Rapid ascent causes surrounding water pressure to drop sharply, and any trapped air in weakened lung tissue expands faster than it can safely vent — enough force to rupture a bleb outright. Most dive medicine guidelines recommend permanent disqualification from diving after a single pneumothorax episode unless surgical correction has been confirmed.
High-altitude flying presents a more nuanced risk. Commercial cabin pressure is typically maintained at the equivalent of 6,000 to 8,000 feet above sea level, which causes gas in the body to expand by roughly 25-30%. For someone with unresolved blebs or a recent pneumothorax, that expansion can trigger a recurrence mid-flight. Most physicians advise waiting a minimum of two weeks after full resolution — and ideally six weeks — before boarding a plane.
Heavy lifting, intense exercise, and even aggressive coughing have all been documented as triggers, though the evidence is less definitive than many patients assume. Atelectasis risk, by contrast, rises sharply after abdominal or thoracic surgery and during prolonged bed rest — any situation where deep breathing is painful or physically restricted.
Diagnosis and Treatment Options
Doctors can typically confirm a collapsed lung within minutes of a patient arriving in the emergency department. A chest X-ray is the first-line diagnostic tool, revealing air in the pleural space or collapsed lung tissue almost immediately. For smaller or ambiguous cases, a CT scan provides far greater detail and can detect a pneumothorax that a standard X-ray might miss entirely.
Pulse oximetry runs simultaneously — a simple clip on the finger measuring blood oxygen saturation. Physicians also listen for reduced or absent breath sounds on the affected side, a fast and telling clinical sign. In a well-equipped ER, the full diagnostic picture usually comes together in under 30 minutes.
How Doctors Diagnose a Collapsed Lung
Ultrasound is increasingly used in trauma bays as a rapid bedside option — studies have shown it can detect pneumothorax with high sensitivity when performed by trained clinicians. According to the American College of Emergency Physicians, point-of-care ultrasound has become a standard adjunct in chest trauma evaluation. It’s faster than waiting for a formal radiology read and doesn’t expose the patient to additional radiation.
Treatment: From Observation to Surgery
Treatment is matched directly to severity. A small primary spontaneous pneumothorax in an otherwise healthy young adult — typically defined as less than 2 cm of air at the lung apex — may require nothing more than watchful waiting, supplemental oxygen, and a follow-up X-ray within 24 to 48 hours.
| Approach | Best Suited For | Key Detail |
|---|---|---|
| Watchful waiting | Small primary spontaneous pneumothorax | Oxygen accelerates natural reabsorption of pleural air |
| Needle aspiration | Moderate primary pneumothorax | Less invasive than chest tube; may avoid hospital admission |
| Chest tube (thoracostomy) | Large or secondary pneumothorax, tension pneumothorax | Tube inserted between ribs to drain air continuously |
| Surgery (VATS or open) | Recurrent pneumothorax, persistent air leak | Video-assisted thoracoscopic surgery can also perform pleurodesis to prevent recurrence |
Tension pneumothorax sits in a category of its own. Air enters the pleural space but cannot escape, building pressure that compresses the heart and great vessels — a rapidly fatal process without immediate needle decompression. This is not a condition managed with observation; it requires emergency intervention within minutes, not a scheduled procedure.
For atelectasis, the treatment path diverges sharply from pneumothorax. Incentive spirometry, chest physiotherapy, and treating the underlying cause — such as clearing a mucus plug or managing post-surgical pain so patients can breathe deeply — are the primary interventions. No chest tube required.
Recovery Timeline and Recurrence Prevention
Recovery from a collapsed lung follows a surprisingly variable timeline depending on the type, severity, and treatment method. Most patients with a small primary spontaneous pneumothorax treated conservatively recover within one to two weeks. Chest tube patients typically spend three to five days in the hospital, with full recovery stretching to four to six weeks before unrestricted physical activity is safe.
What Recovery Actually Looks Like
The first week post-treatment is dominated by soreness at the tube insertion site (if applicable), shallow breathing due to pain, and fatigue that feels disproportionate to the amount of rest taken. Supplemental oxygen may continue at home for patients with lower baseline lung function. Most patients can return to desk work within one to two weeks, but physically demanding jobs require four to six weeks off.
| Milestone | Conservative Treatment | Chest Tube / Surgery |
|---|---|---|
| Pain manageable without opioids | 3-5 days | 7-14 days |
| Return to desk work | 1 week | 2-3 weeks |
| Light exercise (walking) | 1-2 weeks | 3-4 weeks |
| Full physical activity | 2-3 weeks | 4-6 weeks |
| Air travel cleared | 2 weeks minimum | 6 weeks recommended |
Surgical patients — particularly those who undergo video-assisted thoracoscopic surgery (VATS) with pleurodesis — face a longer initial recovery but benefit from significantly lower recurrence rates. VATS involves small incisions, a camera-guided repair of the bleb or leak, and often mechanical or chemical pleurodesis to fuse the lung surface to the chest wall.
Preventing Recurrence
Recurrence is the statistic most patients underestimate. After a first primary spontaneous pneumothorax treated conservatively, approximately 30-50% of patients experience a second episode within one to three years. After a second episode, the probability of a third jumps above 50%. That escalating risk is precisely why many pulmonologists recommend surgical intervention after a second occurrence rather than waiting for a third.
Pleurodesis — either chemical (using talc or doxycycline to irritate the pleural surfaces into fusing together) or mechanical (abrasion during VATS) — drops the recurrence rate to roughly 5% or less. For patients whose anatomy makes them prone to blebs, this is the closest thing to a permanent fix.
Smoking cessation is the single most impactful lifestyle change. Continuing to smoke after a pneumothorax roughly quadruples the recurrence risk compared to quitting entirely. Avoiding rapid altitude changes, including unpressurized aircraft and scuba diving, is also standard medical advice until a pulmonologist clears you — and in some cases, permanently.
Frequently Asked Questions
Can a collapsed lung heal on its own?
A small pneumothorax — typically less than 2 cm of air visible at the lung apex on X-ray — can resolve without intervention. The body gradually reabsorbs the trapped air over one to two weeks. Supplemental oxygen speeds the process by creating a concentration gradient that pulls nitrogen from the pleural space. Larger collapses require active treatment; they will not resolve safely on their own.
How painful is a collapsed lung?
Pain varies widely. Primary spontaneous pneumothorax in a young, healthy person often produces a sharp but tolerable chest pain that some patients mistake for a muscle strain. Secondary pneumothorax in someone with COPD can feel crushing and is accompanied by severe breathing difficulty. Tension pneumothorax produces escalating, agonizing chest pressure as the trapped air compresses the heart. Post-treatment pain from chest tube insertion typically lasts one to two weeks and is manageable with over-the-counter medication in most cases.
Can you die from a collapsed lung?
Most collapsed lungs are not fatal. Primary spontaneous pneumothorax in otherwise healthy individuals has an extremely low mortality rate. Tension pneumothorax, however, is a genuine life-threatening emergency — without immediate treatment, the progressive pressure on the heart can cause cardiovascular collapse and death within minutes. Secondary spontaneous pneumothorax in patients with severe underlying lung disease also carries meaningful mortality risk because their respiratory reserve is already compromised.
How long does it take to recover from a collapsed lung?
Small pneumothorax treated with observation: one to two weeks. Chest tube drainage: three to six weeks for full recovery, with hospital stays averaging three to five days. Surgical repair (VATS with pleurodesis): four to six weeks total, though the long-term outcome is better because recurrence drops below 5%. Most patients return to normal daily activities within two to three weeks regardless of treatment method, but strenuous exercise and air travel require longer clearance periods.
Is a collapsed lung the same as a punctured lung?
Not exactly, though the terms overlap. A punctured lung specifically refers to traumatic pneumothorax — where a physical injury (broken rib, stab wound, medical procedure) creates a hole that allows air to escape into the pleural cavity. A collapsed lung is the broader category that includes both pneumothorax (traumatic and spontaneous) and atelectasis (airway blockage). Every punctured lung causes a collapse, but not every collapsed lung involves a puncture.
Can stress cause a collapsed lung?
Psychological stress alone does not cause a pneumothorax. The condition requires either a structural weakness (blebs), underlying lung disease, or physical trauma. However, stress-related behaviors can be indirect contributors — hyperventilation during a panic attack can theoretically strain already-weakened lung tissue, and stress-related smoking increases long-term risk substantially. Patients who’ve had a pneumothorax commonly experience significant anxiety about recurrence, which is a real and valid concern that physicians increasingly recognize as part of post-treatment care.
A collapsed lung is manageable — even the frightening ones. The critical distinction between pneumothorax and atelectasis determines everything about urgency, treatment, and long-term outlook. Tension pneumothorax demands 911 and immediate intervention. A small spontaneous pneumothorax may heal with nothing more than rest and oxygen. Recovery timelines are predictable, recurrence is preventable with the right approach, and the vast majority of patients return to full, unrestricted lives. The most important thing any patient can do is recognize the warning signs early and not talk themselves out of going to the ER when something feels wrong in the chest.




